Muscular and Neural Anatomy
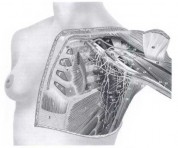
The important muscles in the region of the breast are the pectoralis major and minor, serratus anterior, and latissimus dorsi muscles, as well as the aponeurosis of the external oblique and rectus abdominis muscles (see Fig. 1-2).
{kind=link}
The pectoralis minor muscle arises from the outer aspect of the third, fourth, and fifth ribs and is inserted into the medial border of the upper surface of the coracoid process of the scapula. The muscle is usually prefixed, rather than postfixed, and is innervated by the medial pectoral nerve, which arises mainly from the medial cord of the brachial plexus (G-8, T-1 segmental origin) and descends posteriorly to the muscle crossing the axillary vein anteriorly.
The nerve enters the interpectoral space, passing through the muscle itself in 62% of cases and around the lateral border as a single branch in 38% of cases. Varying numbers of branches passing through the muscle provide motor supply to the lateral part of the pectoralis major muscle. The terms medial and lateral pectoralnerves are confusing: The standard terminology refers to their brachial plexus origin rather than their anatomic positions. Changes in terminology have been proposed but have not yet been generally accepted. The arrangement of these nerves is of particular importance in performing the modified radical (Patey) mastectomy.
The serratus anterior muscle stabilizes the scapula on the chest wall. The muscle arises by a series of digitations from the upper eight ribs laterally; its origin from the first rib is in the posterior triangle of the neck. At its origin from the fifth, sixth, seventh, and eighth ribs, it interdigitates with the origin of the external oblique muscle. The muscle inserts into the vertebral border of the scapula on its costal surface and is supplied by the long thoracic nerve of Bell (the nerve to the serratus anterior muscle). The origin of this important nerve is the posterior aspect of the C-5, C-6, and C-7 roots of the brachial plexus. It passes posteriorly to the axillary vessels, emerging on the chest wall high in the medial part of the subscapular fossa. The nerve lies superficial to the deep fascia overlying the anterior serratus muscle and marks the posterior limit of dissection of the deep fascia. Preservation of the nerve to the serratus anterior muscle as it passes downward is essential to avoid “winging” of the scapula and loss of shoulder power.
The latissimus dorsi muscle, the largest muscle in the body, is characterized by a wide origin from the spinous processes and supraspinous ligaments of the seventh thoracic vertebra downward, including all the lumbar and sacral vertebrae. The muscle inserts, by a narrow tendon forming the posterior axillary fold, into a 2.5-cm insertion in the bicipital groove of the humerus. As the muscle spirals around the teres major muscle, the surfaces of the muscle become reversed to the point of insertion. The muscle is supplied by the thoracodorsal nerve (the nerve to the latissimus dorsi muscle), which arises from the posterior cord of the brachial plexus, with segmental origin from C-6, C-7, and C-8. The nerve passes behind the axillary vessels, approaches the subscapular vessels from the medial side, and then crosses anterior to these vessels to enter the medial surface of the muscle. The nerve passes through the axilla and is intimately involved in the scapular group of lymph nodes. Resection of the nerve does not result in any important cosmetic or functional defect; nevertheless, it should be preserved when possible.
An important landmark in the apex of the axilla is the origin of the subclavius muscle, which arises from the costochondral junction of the first rib. At the tendinous part of the lower border of this muscle, two layers of the clavipectoral fascia fuse together to form a well-developed band, the costocoracoid ligament, which stretches from the coracoid process to the first costochondral junction (the Halsted ligament). At this point, the axillary vessels (the vein being anterior to the artery) enter the thorax, passing over the first rib and beneath the clavicle. Many unnamed small branches of the axillary vein pass to its lower border from the axilla. Near the apex, a small artery, the highest thoracic artery, arises from the axillary artery and lies on the first and second ribs.
M. P. Osborne: Department of Surgery, Joan and Sanford I. Weill Medical College, Cornell University
New York Presbyterian Hospital, New York, New York