Health Centers > Cancer Health Center > Oropharyngeal Cancer
Cancer of the Oropharynx - Oropharyngeal Cancer
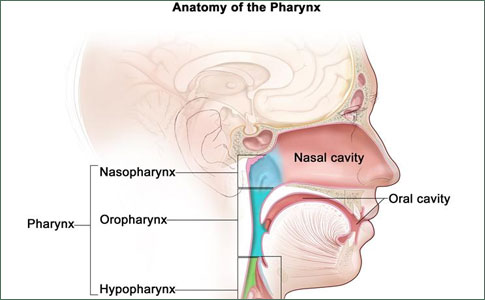
The oropharynx extends from the hard palate superiorly to the hyoid bone inferiorly. The subsites of the oropharynx are (1) the anterior surface of the soft palate, including the uvula; (2) the posterior pharyngeal wall; (3) the anterior and posterior tonsillar pillars; (4) the tonsils and tonsillar fossas; and (5) the posterior one-third of the tongue, which lies between the circumvallate papillae and the vallecula. The lingual surface of the epiglottis is part of the supraglottic larynx. The mucosa of the oropharynx consists of stratified squamous epithelium.
Oropharyngeal Cancer
Anatomy
Pathology
Clinical Findings
Treatment
¬ Primary Cancer
¬ Management of Neck Metastases
Prognosis
References
Pathology
Most oropharyngeal cancers are squamous cell carcinomas, but they tend to be less well differentiated than oral cancers. Deep infiltration is common. Minor salivary gland cancers and lymphomas-partic-larly non-Hodgkin's lymphoma involving the tonsil and other parts of Waldeyer's ring-also arise in this area. Tumors of the parapharyngeal space may also present as oropharyngeal swellings, causing the mucosa of the lateral pharyngeal wall or soft palate to bulge. These are most often retromandibular parotid tumors or neurogenic tumors (eg, neurilemmoma, neurofibroma, or paraganglioma).
The oropharynx is richly supplied with lymphatics. Posterior pharyngeal wall cancers drain bilaterally to jugular chain nodes (levels II, III, and IV) and the retropharyngeal nodes of Ranvier. Cancers of the tonsillar region drain primarily to the upper and mid jugular chain nodes and to the submandibular nodes (levels I, II, and III). Posterior triangle lymph nodes (level V) become involved following involvement of the jugular chain nodes. The overall incidence of cervical lymph node involvement from cancer of the oropharynx is approximately 70%. Bilateral cervical lymph node metastases are common (50%).
Clinical Findings
Patients with cancer of the oropharynx usually present with ulcerating cancers. Cervical lymph node metastases are a common presenting sign. Approximately 70% of patients with tongue base cancers present with advanced cancer, compared with only 35% of patients with cancer of the oral tongue. Tongue base cancers can spread laterally to involve the mandible, anteriorly to involve the oral tongue, and inferiorly to involve the vallecula and supraglottic larynx. Cancers of the tonsillar region readily extend to the mandible. They can also infiltrate the pterygoid muscles, producing trismus. This is an important presenting symptom, and it may limit access for examination. Referred otalgia is common with deeply infiltrating cancers.
T STAGE: OROPHARYNGEAL CANCER
T1 Tumor 2 cm or less in greatest dimension T2 Tumor more than 2 cm but not more than 4 cm in greatest dimension T3 Tumor more than 4 cm in greatest dimension T4 Tumor invades adjacent structures (eg, through cortical bone, into deep [extrinsic] muscle of tongue, maxillary sinus, skin)
Treatment
A. Primary Cancer
Treatment for cancer of the oropharynx must be individualized. For small cancers (T1 and T2), surgery or radiation therapy gives similar results. For these cancers, surgical access can be achieved through the open mouth or by splitting the lower lip and jaw and retracting the mandible laterally (mandibular swing procedure). Excision of a soft palate cancer is readily accomplished, but when the muscular continuity of the soft palate is completely disrupted, regurgitation of food into the nasal cavity occurs. Therefore, small cancers are usually treated with radiation therapy and surgery is reserved for advanced or recurrent cancer.
Anal Cancer: Strategies in Management
The management of anal cancer underwent an interesting transformation over the last two decades.
For more advanced cancers, the choices for therapy are (1) surgery combined with postoperative radiation therapy and (2) initial radiation therapy followed by surgery in the event of recurrence. Combined therapy offers the best chance of local cancer control. Total glossectomy may be necessary to encompass large cancers of the tongue base. Tongue base cancers that extend beyond the vallecula require glossectomy and laryngectomy to remove the cancer completely and to prevent subsequent aspiration pneumonia. Operative defects can be repaired with skin grafts, pedicled myocutaneous flaps (pectoralis major flap), or free flaps (radial forearm and osteomyocutaneous fibular free flaps). Temporary tracheotomy is mandatory in these circumstances.
B. Management of Neck Metastases
Cervical lymph node metastases are treated by radical or modified neck dissection. If the neck is clinically free of cancer, an elective supraomohyoid neck dissection or radiation therapy is appropriate. If the primary cancer is treated by radiation therapy, the cervical lymph nodes at risk are included in the radiation field. If the primary cancer is treated surgically, an elective neck dissection is appropriate. If postoperative radiation therapy is planned for the primary cancer site, it is reasonable to include the neck in the radiation field instead of performing an elective neck dissection. Initial (induction, neoadjuvant) chemotherapy using cisplatin, fluorouracil, and paclitaxel, singly or in combination, gives response rates of up to 80%, but these responses are rarely of long duration.
Prognosis
The 5-year survival rates for cancer of the oropharynx with appropriate treatment are as follows: stage I, 75%; stage II, 65%; stage III, 45%; and stage IV, less than 30%. Quality of life is a major consideration in the treatment of oropharyngeal cancers, since swallowing and speech are often adversely affected by treatment.
The clinical staging of oropharyngeal cancers depends primarily on tumor size and is similar to the staging of oral cavity cancers (Table 90-8). Although tumors may arise from any site in the oropharynx, they arise most commonly from the palatine arch, which includes the tonsillar fossa and base of the tongue. The most common presenting symptom is chronic sore throat (often unilateral) and referred otalgia.
Change in voice, dysphagia, and trismus are late signs. Regional lymphatic metastases occur frequently and are related to the depth of tumor invasion and tumor size. Upper cervical nodes are generally first involved, but lower nodes can become clinically involved with skipping of the upper first-echelon nodes. Bilateral lymphatic metastases can occur, particularly with cancers of the soft palate, tongue base, and midline pharyngeal wall » »
References
Forastiere AA et al: Radiotherapy and concurrent chemotherapy: a strategy that improves locoregional control and survival in oropharyngeal cancer. J Natl Cancer Inst 1999;91:2065. Pubmed: 10601369
Harrison LB et al: Current philosophy on the management of cancer of the base of the tongue. Oral Oncol 2003;39:101. Pubmed: 12509962
Parsons JT et al: Squamous cell carcinoma of the oropharynx. Cancer 2002;94:2967. Pubmed: 12115386
