Health Centers > Cancer Health Center > Cancer of the Nasal Cavity
Cancer of the Nasal Cavity
Anatomy
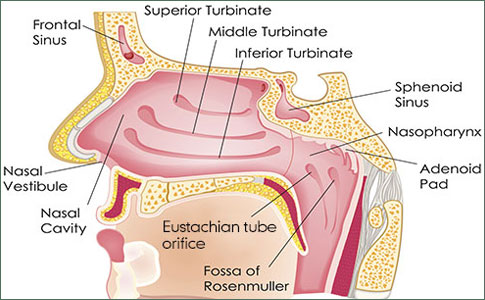
The nasal cavity is divided into right and left nasal fossae by the nasal septum. Each fossa has an anterior opening (naris or nostril), a posterior opening (choana), and bony projections called turbinates protruding from the lateral walls. Posterior to the nasal cavity is the nasopharynx. Its roof is formed by the skull base, which slopes downward and backward, while the inferior limit is a posterior extension of the plane of the hard palate. The lateral wall is composed of the torus tubularis, the auditory tube orifice, and Rosenmuller's fossa. The paranasal sinuses consist of the maxillary and ethmoid sinuses bilaterally, the frontal sinus, and the sphenoid sinus. Each maxillary sinus shares a common wall with the orbit above, the nasal cavity medially, the oral cavity inferiorly, and the infratemporal fossa posteriorly.
Cancer of the Nasal Cavity, Napopharynx, and Paranasal Sinuses
Anatomy
Pathology
Clinical Findings
Diagnosis
Treatment
Prognosis
References
The mucosa of the nasal cavity consists of ciliated pseudostratified columnar epithelium (respiratory mucosa) except in the region of the superior turbinate and the adjacent lateral wall and septum, which is lined by specialized nonciliated epithelium (olfactory mucosa). The sinuses are lined by respiratory epithelium, and melanocytes are scattered throughout the region. The nasopharynx is lined by respiratory epithelium in early life, but squamous metaplasia occurs with aging so that about 60% of the respiratory mucosa is replaced by squamous epithelium in the first decade of life. Initially, this squamous epithelium is nonkeratinizing, but after age 50 more keratinization occurs.
Pathology
The most common cancer of the nasal cavity and paranasal sinuses is squamous cell carcinoma. The maxillary antrum is the most common site, while cancers of the nasal cavity are rare. Adenocarcinoma, sarcoma, melanoma, lymphoma, and minor salivary gland cancers also occur. Esthesioneuroblastoma is an uncommon cancer that arises from olfactory mucosa at the superior aspect of the nasal cavity. It readily invades the ethmoid sinuses and can involve the orbit. In the nasopharynx, squamous carcinomas, 80% of which are nonkeratinizing, also predominate. Lymphoepithelioma, a subgroup of nonkeratinizing squamous carcinoma, is poorly differentiated, lacks squamous or glandular differentiation, and has a lymphocytic component. It is highly radiosensitive.
Cancers of the skin of the vestibule of the nose can drain to parotid, submandibular, or upper jugular nodes (levels I and II). Nasal cavity and maxillary sinus cancers rarely metastasize to the regional lymph nodes unless they are advanced and have invaded adjacent structures. The nasopharynx is richly supplied with lymphatics, and cancers in this region readily drain bilaterally to upper and mid jugular lymph nodes and to posterior triangle lymph nodes (levels II, III, and V). Cervical lymph node metastases occur in 80% of patients with this cancer. Palpable cervical lymphadenopathy is the initial manifestation of 50% of patients with nasopharyngeal cancer. Unlike other squamous cell carcinomas, cancers of the nasopharynx can metastasize to the posterior triangle (level V) in the absence of jugular lymph node involvement.
Anal Cancer: Strategies in Management
The management of anal cancer underwent an interesting transformation over the last two decades.
Clinical Findings
Cancers of the nasal cavity, paranasal sinuses, and nasopharynx are frequently advanced at presentation. Early symptoms such as nasal obstruction, nasal discharge, and sinus congestion are so commonly associated with benign conditions that they are not frequently investigated for the presence of a cancer. Hemorrhage can occur. Bone invasion and involvement of adjacent soft tissue structures are common. Along with the tonsillar fossa, the tongue base, and the piriform sinus, the nasopharynx is an important site of clinically occult primary cancer. Cancers of the maxillary sinus can invade the hard palate and enter the oral cavity. They can also invade the orbital floor, causing visual symptoms and proptosis. Anterior invasion through the skin can occur. In advanced maxillary sinus cancers, cervical lymph node metastases can be the initial manifestation. Cranial nerve symptoms result from invasion of the skull base.
Cancer of the Oral Cavity
Anatomy
Pathology
Clinical Findings
Treatment
¬ Primary Cancer
¬ Management of Neck Metastases
Prognosis
Diagnosis
Diagnosis and assessment of the extent of cancer are more difficult for cancers in this area than for those elsewhere in the upper aerodigestive tract. Histologic examination of an adequate tissue biopsy specimen is always required. CT scanning is performed to delineate the extent of the cancer, though it can be difficult to differentiate between cancer and edematous mucosa. MRI is helpful in making this differentiation.
T STAGE: MAXILLARY SINUS CANCER
T1 Tumor limited to antral mucosa with no erosion or destruction of bone T2 Tumor with erosion or destruction of the infrastructure, including the hard palate or middle nasal meatus T3 Tumor invades any of the following: skin of cheek, posterior wall of maxillary sinus, floor or medial wall of orbit, anterior ethmoid sinus T4 Tumor invades orbital contents and/or any of the following: cribriform plate, posterior ethmoid or sphenoid sinuses, nasopharynx, soft palate, pterygomaxillary or temporal fossas or base of skull
Treatment
Radiation is the principal treatment method for cancer of the nasopharynx. Undifferentiated cancers respond better than well-differentiated ones, and treatment is more successful in younger patients. A dose of 7000 cGy is usually required for the primary cancer. Both sides of the neck are treated because of the high incidence of bilateral cervical lymph node metastases.
The Nasopharynx - nasopharyngeal carcinoma
In the United States, nasopharyngeal carcinoma (NPC) accounts for 2% of all HNSCCs. Its unusual epidemiologic and natural history features include a remarkable tendency toward early regional and distant dissemination. NPC also is extremely sensitive to radiotherapy and cytotoxic chemotherapy.
In the adult, the nasopharynx is a chamber that is approximately cuboidal in shape and 4 cm on an edge. It is bounded anteriorly by the choana of the nasal cavity, superiorly by the clivus, and inferiorly by the soft palate. Its posterior wall is the mucosa that overlies the superior constrictor muscles of the pharynx and the C1 and C2 vertebral bodies. The lateral walls contain the Eustachian tube orifices » »
Cancers of the maxillary sinus are treated by maxillectomy. For advanced (T3, T4) maxillary sinus cancers, surgery and postoperative radiation therapy provide for the best local control. Orbital exenteration is necessary for maxillary cancers that invade the periorbital tissues. Because the incidence of cervical lymph node metastases is low with cancers of the paranasal sinuses, prophylactic neck dissection or radiation therapy is not necessary. Resectable cancers of the upper nasal cavity and ethmoid sinuses require craniofacial excision, which entails frontal craniotomy to assess the extent of the intracranial extension of the cancer.
Nose and Paranasal Sinuses cancers
As mentioned previously, the nose and the paranasal sinuses pose a unique set of problems that deserve separate consideration from SCC of the UADT. For instance, while SCC is still the most common histology found there, it accounts for less than 50% of disease. The four most common malignant histologies of the paranasal sinuses are SCC, sinonasal undifferentiated carcinoma (SNUC), neuroendocrine carcinoma, and esthesioneuroblastoma (often referred to as olfactory neuroblastoma).
Cancer of the nose and paranasal sinuses is relatively rare. When taken as a whole, these malignancies account for only 0.2% to 0.8% of cancers diagnosed annually, or approximately 3% of cancers of the UADT. The incidence is generally reported as 0.3 to 1 per 100,000 population. These cancers tend to occur most commonly in the fifth decade of life although they can occur in the much younger and much older. Cancer of the nose and paranasal sinuses is rare in children except for some sarcomas, such as rhabdomyosarcoma. While there are numerous environmental factors associated with cancer of the nose and paranasal sinuses, as industry has modernized, these have become somewhat less important. There continues to be a relationship between these malignancies and tobacco exposure, however » »
Prognosis
Five-year survival rates for nasopharyngeal cancer with appropriate treatment are as follows: stage I, 85%; stage II, 75%; stage III, 45%; stage IV, 10%. One-third of patients die of distant metastases.
Five-year survival rates for maxillary sinus cancer with appropriate treatment are as follows: stage I, 85%; stage II, 65%; stage III, 40%; stage IV, 15-20%.
References
Oh JL et al: Induction chemotherapy followed by concomitant chemoradiotherapy in the treatment of locoregionally advanced nasopharyngeal cancer. Ann Oncol 2003;14:564. Pubmed: 12649102
