Health Centers > Cancer Health Center > Cancer of the Hypopharynx
Cancer of the Hypopharynx
The hypopharynx extends from the hyoid bone superiorly to the lower border of the cricoid cartilage inferiorly. It is composed of four subsites: (1) the piriform sinuses, situated lateral to the larynx; (2) the postcricoid area, lying immediately behind the larynx; (3) the posterior pharyngeal wall; and (4) the marginal area where the medial wall of the piriform sinus and the false vocal cord meet superiorly at the aryepiglottic fold. Laterally, the piriform sinuses are bounded by the alae of thyroid cartilage and the thyrohyoid membrane. The hypopharynx, lined by stratified squamous epithelium, has a muscular wall consisting of the middle and inferior constrictor muscles. The retropharyngeal space posterior to the hypopharynx, which contains lymphatics and loose areolar tissue, separates the visceral compartment of the neck from the prevertebral muscles with their overlying prevertebral fascia.
Pathology
Hypopharyngeal Cancer
Anatomy
Pathology
Clinical Findings
Treatment
¬ Primary Cancer
¬ Management of Neck Metastases
Prognosis
References
Over 95% of hypopharyngeal cancers are squamous carcinomas, which usually present as infiltrating ulcerative lesions. The incidence of poorly differentiated cancer is higher in the hypopharynx than in other regions. The size of these cancers can be deceptive on clinical evaluation because of submucosal lymphatic extension. Minor salivary gland cancers and lymphomas occasionally occur in the hypopharynx, where they usually present as submucosal tumors. Benign hypopharyngeal lesions include webs, strictures, and pharyngoesophageal (Zenker's) diverticula.
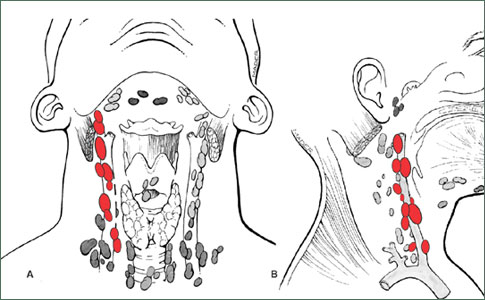
Cancer of the hypopharynx has a high propensity for lymphatic invasion, with most patients having cervical lymph node metastases at the time of initial presentation. The hypopharynx-especially the piri-orm sinus-must always be examined in an adult with cervical lymph node metastases and no obvious primary cancer site. Occult cervical lymph node metastases (ie, clinically negative but histologically positive) are also common, causing the overall incidence of cervical lymph node metastases at presentation to be approximately 75%. The principal cervical lymph node groups involved are the upper, mid, and lower jugular nodes (levels II, III, and IV); the retropharyngeal nodes of Ranvier; and, less frequently, the cervical lymph nodes along the spinal accessory nerve in the posterior triangle (level V).
Clinical Findings
The most common site for hypopharyngeal cancer is the piriform sinus, accounting for 60% of cases. The postcricoid region is affected in 25% of patients and the posterior pharyngeal wall in 15%. Postcricoid lesions are frequently circumferential and cause dysphagia, while piriform sinus lesions tend to remain silent for a long time. Patients with hypopharyngeal cancer are typically men in their fifth to eighth decades with a history of excessive alcohol and tobacco use.
The chief symptoms of hypopharyngeal cancer are pain, dysphagia, and weight loss. Pain can be localized to the site of the cancer or can be referred to the ipsilateral ear. About 25% of patients, especially those with lesions of the piriform sinus, present with palpable cervical lymphadenopathy and no other symptoms. Advanced cancers can invade the larynx and cause vocal cord paralysis and hoarseness. Direct laryngopharyngoscopy and biopsy are necessary to confirm the diagnosis and assess the extent of the cancer.
Anal Cancer: Strategies in Management
The management of anal cancer underwent an interesting transformation over the last two decades.
T STAGE: HYPOPHARYNGEAL CANCER
T1 Tumor limited to one subsite of the hypopharynx and 2 cm or less in size T2 Tumor invades more than one subsite of the hypopharynx or an adjacent site, or measures more than 2 cm and no more than 4 cm in size, without fixation of the hemilarynx T3 Tumor invades more than one subsite of the hypopharynx or an adjacent site, with fixation of the hemilarynx T4 Tumor invades adjacent structures (eg, cartilage or soft tissues of the neck)
Hypopharyngeal cancer is a term used for tumors of a subsite of the upper aerodigestive tract, and like most other subsite designations, the distinction is anatomic rather than pathophysiologic within the group of head and neck malignancies. The hypopharynx is the region between the oropharynx above (at the level of the hyoid bone) and the esophageal inlet below (at the lower end of the cricoid cartilage). Embryologically, the larynx interjects into the hypopharynx anteriorly and is therefore considered a separate structure.
Hypopharyngeal cancers are often named for their location, including pyriform sinus, lateral pharyngeal wall, posterior pharyngeal wall, or postcricoid pharynx (see images below). Most arise in the pyriform sinus. In the United States and Canada, 65-85% of hypopharyngeal carcinomas involve the pyriform sinuses, 10-20% involve the posterior pharyngeal wall, and 5-15% involve the postcricoid area.
Treatment
The goals of treatment are to cure the cancer and maintain functional continuity of the upper aerodigestive tract. Intensive nutritional therapy is necessary if long-standing dysphagia has resulted in cachexia. Patients with cancer of the hypopharynx also commonly have pulmonary disease that must be assessed and managed preoperatively.
A. Primary Cancer
Surgical resection of hypopharyngeal cancers usually requires laryngopharyngectomy. Small (T1, T2) cancers of the piriform sinuses are curable with radiation therapy. Small (T1 and T2) cancers of the posterior pharyngeal wall can be treated with larynx-preserving local excision. Jejunal and tubed radial forearm free flaps permit excellent hypopharyngeal reconstruction. If a cancer extends to or arises in the cervical esophagus, laryngopharyngectomy and esophagectomy may be required. In this circumstance, a gastric pull-up procedure provides for upper aerodigestive tract continuity.
Frequency
Cancer that arises in the hypopharynx represents approximately 7% of all cancers of the upper aerodigestive tract. The incidence of laryngeal cancer is 4-5 times that of hypopharyngeal cancer. All pharyngeal subsites accounted for approximately 124,000 cancer cases worldwide in 2002.
An analysis of the Surveillance Epidemiology and End Results (SEER) database demonstrates that the incidence of hypopharyngeal cancers decreased 35% from 1975 to 2001. The mortality rate due to hypopharyngeal cancers also decreased by 30%. This epidemiologic change is believed to be due to a decrease in the initiation of cancer in the hypopharynx and does not necessarily reflect any improvement in survival due to treatment.
Race
African Americans have had an increasing incidence of cancers of all pharyngeal subsites since the early 1970s.
Sex
US incidence indicates an approximate male-to-female ratio of 3:1. Women have a higher incidence of postcricoid cancers related to nutritional deficiencies (Plummer-Vinson syndrome) than men. The prognosis for women generally is better than that for men.
Age
The incidence of hypopharyngeal cancer rises in people older than 40 years; it is rare in people younger than 30 years. The mean age at presentation is 65 years. Patients diagnosed with hypopharyngeal cancer are typically men aged 55-70 years with a history of tobacco use and/or alcohol ingestion.
Prognosis
The biological behavior of carcinoma of the hypopharynx differs greatly from that of carcinoma of the larynx. Carcinomas of the hypopharynx are usually poorly differentiated and patients are usually asymptomatic; early presentations are unfortunately uncommon. In fact, T1 N0 cases (see Staging in Workup) account for only 1-2% of all patients seen.
B. Management of Neck Metastases
The incidence of cervical lymph node metastases is so high with hypopharyngeal cancers that some form of neck treatment is appropriate for all patients. Treatment of both sides of the neck is frequently indicated. Radical or modified neck dissection is indicated for clinically evident cervical lymph node metastases. For the clinically negative neck, when the primary cancer is treated with radiation therapy, the neck is also treated with radiation therapy. If the primary cancer is treated surgically, elective neck dissection is performed. If postoperative radiation therapy will be given to the primary cancer site, radiation therapy can also be given to the neck, making an elective neck dissection unnecessary.
The Hypopharynx - Hypopharyngeal cancers
The hypopharynx represents one of the most lethal sites for SCC. Lymph node metastases are clinically evident at time of diagnosis in 70% to 80% of patients and are indicative of advanced disease. Bilateral and contralateral lymph node metastases occur in 10% to 20% of cases, particularly if tumors cross the midline of the hypopharynx. Primary tumor extension beyond the hypopharynx is common. Hypopharyngeal cancers are characterized by a propensity to spread submucosally to involve the oropharynx or esophagus. Ulcerated deep infiltration and skip areas are common. This leads to difficulties in adequately assessing the margins of the tumor and contributes to poor local tumor control, even with the addition of adjuvant radiation. The majority (more than 75%) of hypopharyngeal cancers arise in the pyriform sinus while 20% occur in the posterior pharyngeal wall. Postcricoid cancers are rare (less than 5% of hypoparyngeal cancers). Posterior pharyngeal wall cancers tend to grow superficially and only involve the prevertebral fascia in advanced lesions. Pyriform cancers spread early to other contiguous structures, such as the larynx, postcricoid area, thyroid gland, and thyroid and cricoid cartilages. Most pyriform sinus cancers arise along the medial wall followed by the lateral wall of the sinus. The postcricoid mucosa is contiguous with the apex of the pyriform and tumor can spread circumferentially to involve the entire lower hypopharynx. Because of the locale of hypopharyngeal cancers and their growth patterns and proximity to the larynx, surgical management often entails total laryngopharyngectomy. » »
Prognosis
In patients with cancer of the hypopharynx, distant metastases appear in 25% of patients-a much higher incidence than with cancers of the oral cavity and oropharynx. The 5-year survival rates for patients with cancer of the hypopharynx receiving appropriate treatment are subsite-specific. Generally, patients with hypopharyngeal cancers do worse than patients with oropharyngeal cancers.
How is hypopharyngeal cancer diagnosed?
Tests and procedures that are used to diagnose hypopharyngeal cancer include:
Endoscopy - This procedure uses a thin, lighted tube that is inserted into the nose or mouth to check for anything unusual.
Physical exam - Doctors check for swollen lymph nodes in the neck and look down the throat with a small mirror to check for anything unusual.
CT scan (also called computed tomography or computerized tomography) - This scan takes a series of detailed pictures of areas inside the body. The images are created by a computer that is linked to an X-ray machine.
MRI (also called magnetic resonance imaging) - This procedure uses radio waves and a powerful magnet, linked to a computer, to create detailed pictures of areas inside the body.
Esophagoscopy - This procedure looks inside the esophagus to check for unusual areas. An esophagoscope (a thin, lighted tube) is inserted through the mouth and down the throat into the esophagus. Tissue samples might be taken for biopsy. This is usually done under general anesthesia or heavy sedation.
Bronchoscopy - This procedure looks for unusual areas inside the trachea and large airways of the lung. A bronchoscope (a thin, lighted tube) is inserted through the nose or mouth into the trachea and lungs. Tissue samples might be taken for biopsy. This is usually done under general anesthesia or heavy sedation.
Biopsy - In this procedure, tissue samples are removal and viewed under a microscope to determine if cancer is present.
References
Chu PY et al: Surgical treatment of squamous cell carcinoma of the hypopharynx: analysis of treatment results, failure patterns, and prognostic factors. J Laryngol Otol 2004;118:443. Pubmed: 15285863
Urba SG et al: Organ preservation for advanced resectable cancer of the base of tongue and hypopharynx: a Southwest Oncology Group Trial. J Clin Oncol 2005;23:88. Pubmed: 15625363
