Updated systemic sclerosis criteria improve disease classification
New classification criteria for systemic sclerosis have just been published and are more sensitive than the 1980 criteria, enabling earlier identification and treatment of this disabling autoimmune disease. The 2013 criteria, developed by a joint committee commissioned by the American College of Rheumatology (ACR) and European League Against Rheumatism (EULAR), are published in the ACR journal, Arthritis & Rheumatism.
Systemic sclerosis, also known as scleroderma, is a connective tissue disease that is characterized by sclerodermatous skin changes – a hardening of tissue due to increased collagen deposits; Raynaud’s phenomenon–spasms of small blood vessels in response to cold or stress that cause color changes in fingers or toes, to obliteration of blood vessels (vasculopathy) leading to tissue death; and internal organ fibrosis–formation of excess tissue that scars organs. The ACR estimates that systemic sclerosis affects 49,000 U.S. adults.
The joint ACR-EULAR committee was led by Dr. Janet Pope from Western University, St. Joseph’s Health Care London in Ontario, Canada, and Dr. Frank van den Hoogen from St. Maartenskliniek in The Netherlands. The committee’s intent was to improve the classification of systemic sclerosis by clustering items and simplifying the weighting of the different criteria. The new criteria set was tested for specificity and sensitivity by comparing scleroderma cases with controls (patients with disorders similar to scleroderma), and validated by experts viewing cases with and without the disease.
“There is a need for improved classification criteria for systemic sclerosis,” explains Dr. van den Hoogen. “The 1980 ACR criteria were not sensitive enough to identify patients with early disease or limited cutaneous system sclerosis. Our efforts with the joint committee addressed this sensitivity issue, resulting in the 2013 classification criteria for systemic sclerosis.”
Based on the new criteria, a patient with thickening of the skin in the middle part of the fingers (from proximal to the metacarpophalangeal joints) would be classified as having systemic sclerosis, regardless of other features. If this criterion was not met, however, then seven items with varying weights would need to be assessed in order to obtain a scleroderma classification: skin thickening of the fingers, fingertip lesions, telangiectasia, abnormal nailfold capillaries, pulmonary arterial hypertension and/or interstitial lung disease, Raynaud’s phenomenon, and SSc-related antibodies.
 The results of the validation testing show that sensitivity and specificity were both greater than 90% for the 2013 systemic sclerosis classification criteria compared to 75% for the 1980 ACR criteria. “The new systemic sclerosis classification criteria should correctly classify more patients with the disease,” concludes Dr. Pope. “Criteria that are more specific will allow for earlier identification and better treatment for those with systemic sclerosis.”
The results of the validation testing show that sensitivity and specificity were both greater than 90% for the 2013 systemic sclerosis classification criteria compared to 75% for the 1980 ACR criteria. “The new systemic sclerosis classification criteria should correctly classify more patients with the disease,” concludes Dr. Pope. “Criteria that are more specific will allow for earlier identification and better treatment for those with systemic sclerosis.”
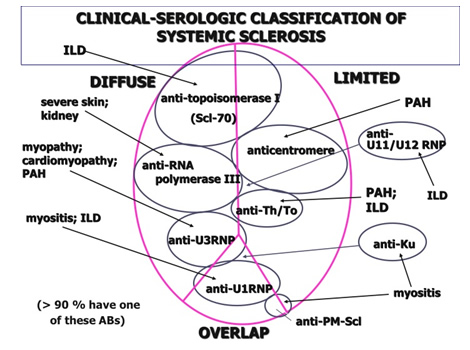
Types of systemic sclerosis
Systemic sclerosis is classified into two main types, according to the extent of skin involvement.
Limited cutaneous systemic sclerosis (lcSSc), or limited scleroderma
- 70% of systemic sclerosis cases.
- Affects only the face, forearms and lower legs up to the knee.
- CREST syndrome (= C alcinosis, R aynaud’s disease, (O)E sophageal dysmotility, S clerodactyly, T elangiectasia) is an older term for limited scleroderma.
Diffuse cutaneous systemic sclerosis (dcSSc), or diffuse scleroderma
- 30% of systemic sclerosis cases.
- Involves also the upper arms, thighs or trunk.
Other types
There are rarer types, including systemic scleroderma sine scleroderma (internal organ involvement without the skin changes).
###
This study is published in Arthritis & Rheumatism. Media wishing to receive a PDF of this article may contact .(JavaScript must be enabled to view this email address).
Full citation: “2013 Classification Criteria for Systemic Sclerosis. An American College of Rheumatology and European League Against Rheumatism Collaborative Initiative” Frank van den Hoogen, Dinesh Khanna, Jaap Fransen, Sindhu R. Johnson, Murray Baron, Alan Tyndall, Marco Matucci-Cerinic, Raymond P. Naden, Thomas A. Medsger Jr., Patricia E. Carreira, Gabriela Riemekasten, Philip J. Clements, Christopher P. Denton, Oliver Distler, Yannick Allanore, Daniel E. Furst, Armando Gabrielli, Maureen D. Mayes, Jacob M. van Laar, James R. Seibold, Laszlo Czirjak, Virginia D. Steen, Murat Inanc, Otylia Kowal-Bielecka, Ulf Mu¨ller-Ladner, Gabriele Valentini, Douglas J. Veale, Madelon C. Vonk, Ulrich A. Walker, Lorinda Chung, David H. Collier, Mary Ellen Csuka, Barry J. Fessler, Serena Guiducci, Ariane Herrick, Vivien M. Hsu, Sergio Jimenez, Bashar Kahaleh, Peter A. Merkel, Stanislav Sierakowski, Richard M. Silver, Robert W. Simms, John Varga and Janet E. Pope. Arthritis & Rheumatism; Published Online: October 3, 2013 (DOI: 10.1002/art.38098).
What are the signs and symptoms of systemic sclerosis?
Raynaud phenomenon is usually the first symptom of systemic sclerosis. Patients experience episodes of vasospasm , which causes blood vessels in the fingers and toes to constrict. As less blood is reaching these extremities the skin changes colour to white and the fingers and toes may feel cold and numb. As they warm up, they go blue and then red before returning to normal again.
Other skin changes include:
Itchy skin
Thickening of the skin of the fingers, then atrophy (thinned) and sclerosis (scarring). The fingers become spindle-shaped (sclerodactyly) from resorption of the fingertips.
Fragile nails become smaller with ragged cuticles
Taut, shiny skin that may have dark or pale patches (hyperpigmentation or hypopigmentation). The tight skin may affect most parts of the body, including the face, resulting in loss of expression and difficulty opening the mouth properly.
Visibly dilated blood vessels (telangiectases) appear on the fingers, palms, face, lips, tongue and chest.
Calcinosis (calcium deposits) develops in the skin, particularly the fingers, hands and other bony areas. These can breakdown and discharge chalky material.
Ulcers may follow minor injuries over the joints, or on the tips of fingers and toes where the circulation is poor. Ulceration can lead to dry gangrene and eventual loss of the tips of the fingers (like frost bite).
Ulcers may also arise over calcinosis and on the lower legs.
Sicca symptoms (dry eyes, dry mouth) and Sjogren syndrome
About the Journal
 Arthritis & Rheumatism is an official journal of the American College of Rheumatology (ACR) and covers all aspects of inflammatory disease. The American College of Rheumatology is the professional organization whose members share a dedication to healing, preventing disability, and curing the more than 100 types of arthritis and related disabling and sometimes fatal disorders of the joints, muscles, and bones. Members include practicing physicians, research scientists, nurses, physical and occupational therapists, psychologists, and social workers. The journal is published by Wiley on behalf of the ACR.
Arthritis & Rheumatism is an official journal of the American College of Rheumatology (ACR) and covers all aspects of inflammatory disease. The American College of Rheumatology is the professional organization whose members share a dedication to healing, preventing disability, and curing the more than 100 types of arthritis and related disabling and sometimes fatal disorders of the joints, muscles, and bones. Members include practicing physicians, research scientists, nurses, physical and occupational therapists, psychologists, and social workers. The journal is published by Wiley on behalf of the ACR.
About Wiley
Wiley is a global provider of content-enabled solutions that improve outcomes in research, education, and professional practice. Our core businesses produce scientific, technical, medical, and scholarly journals, reference works, books, database services, and advertising; professional books, subscription products, certification and training services and online applications; and education content and services including integrated online teaching and learning resources for undergraduate and graduate students and lifelong learners.
Founded in 1807, John Wiley & Sons, Inc. (NYSE: JWa, JWb), has been a valued source of information and understanding for more than 200 years, helping people around the world meet their needs and fulfill their aspirations. Wiley and its acquired companies have published the works of more than 450 Nobel laureates in all categories: Literature, Economics, Physiology or Medicine, Physics, Chemistry, and Peace. Wiley’s global headquarters are located in Hoboken, New Jersey, with operations in the U.S., Europe, Asia, Canada, and Australia.