Health Centers > Sexual Health Center > Sexually Transmitted Diseases > Syphilis
Syphilis
Syphilis is caused by the spirochete Treponema pallidum. The infection is transmitted by contact with infectious mucocutaneous lesions primarily through sexual contact, although indirect evidence suggests syphilis may be spread by the practice of sharing needles among intravenous drug users. The reported rate of syphilis in the United States is at its lowest level since reporting began in 1941. However, the genital ulcers of syphilis increase the risk of transmission of HIV, making it an STD of continued significance.
SYPHILIS
Natural History & Principles of Diagnosis & Treatment
Introduction
Laboratory Diagnosis
Treatment
Complications of Specific Therapy
Follow-Up Care
Prevention
Course & Prognosis
Clinical Stages of Syphilis
Primary Syphilis
¬ Essentials of Diagnosis
¬ General Considerations
¬ Laboratory Findings
¬ Differential Diagnosis
¬ Treatment
Secondary Syphilis
Relapsing Syphilis (Early Latent Syphilis)
Late Latent ("Hidden") Syphilis
Late (Tertiary) Syphilis
Syphilis in HIV Infected Patients
Syphilis in Pregnancy
Congenital Syphilis
The incidence of syphilis increased in the United States through the 1980s peaked in 1990, and then subsequently declined (Centers for Disease Control and Prevention, 2003a). The rate of syphilis in the United States in 2002 was 2.4 cases per 100,000 persons, and the rate among neonates was even lower at 1.1 cases per 100,000 population. The Centers for Disease Control and Prevention created a National Syphilis Elimination Plan with a goal of fewer than 1000 cases of primary and secondary syphilis in the country by 2005 (Mitka, 2000).
Increased rates of maternal syphilis have been linked to substance abuse, especially crack cocaine, and to inadequate prenatal care (Lago, 2004; Minkoff, 1990; Warner, 2001, and all their colleagues). Klass and associates (1994), in a study of prenatal syphilis at the Boston City Hospital during four decades, concluded that the continued prevalence of syphilis at delivery was associated with substance abuse, HIV infection, lack of prenatal care, treatment failures, and reinfection.
Antepartum syphilis can profoundly affect pregnancy outcome by causing preterm labor, fetal death, and neonatal infection by transplacental or perinatal infection (Genc and Ledger, 2000; Watson-Jones and co-workers, 2002). Fortunately, of the many congenital infections, syphilis is the most readily prevented and the most susceptible to therapy.
Clinical Presentation
Primary Syphilis
The classic chancre of primary syphilis appears about 21 days after exposure. The chancre is an indurated, painless ulcer usually located on the genitalia but also found at other sites of sexual contact including the cervix, breast, mouth, anus, or vaginal canal. The primary lesion heals spontaneously. Because the chancre is painless the primary stage of syphilis may be undetected.
Secondary Syphilis
Hematogenous spread of T. pallidum produces the symptoms of secondary syphilis. Some patients are asymptomatic while others have constitutional symptoms including fever, malaise, and generalized lymphadenopathy. A macular, papular, annular, or follicular rash classically is present on the palms of the hands and soles of the feet. Mucous patches are shallow, painless ulcerations found on mucous membranes. Broad, raised, grayish, papular lesions known as condylomata lata appear on moist body areas such as the genitalia, cervix, scrotum, anus, or inner thighs. Alopecia may also be present. The signs and symptoms of secondary syphilis resolve spontaneously, after which the patient enters the latent stages of syphilis.

Male Infertility
Primary infertility affects 15-20% of married couples. Approximately one-third of cases ...







Latent Syphilis
The first year of untreated infection is known as early latent syphilis. During this time, infectious mucocutaneous symptoms of secondary syphilis recur in approximately 25% of untreated patients with recurrences taking place up to 5 years after infection. Late latent syphilis or syphilis of unknown duration occurs after the first year of untreated infection.
During this time the patient has a positive specific treponemal antibody test but usually no other signs or symptoms of disease.
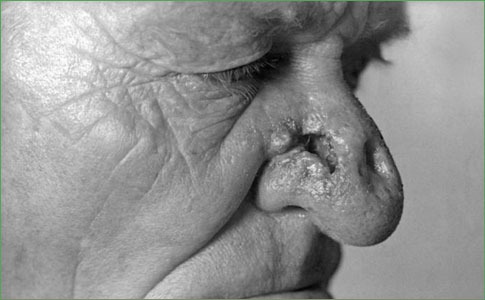
Late (Tertiary) Syphilis
One third of men and women with untreated syphilis go on to develop tertiary syphilis, which includes cardiovascular syphilis, gummatous syphilis, and neurosyphilis. It is important to note that neurosyphilis is not confined only to the tertiary stage. Cardiovascular problems include aortitis, aortic regurgitation, and aortic aneurysm. Gummas are granulomatous-like lesions that infiltrate the skin, soft tissues, bone, liver, and other organ systems.
Neurosyphilis
Neurosyphilis can occur any time after the primary infection. Central nervous system (CNS) involvement by syphilis is often asymptomatic. Historically, 4% to 9% of patients with untreated syphilis develop symptomatic neurosyphilis. Patients with neurosyphilis have a number of clinical syndromes. Meningeal syphilis usually occurs during the first year of infection and is characterized by headache, stiff neck, nausea, and vomiting. Cranial nerve involvement can result in hearing loss, facial weakness, or visual disturbances. Syphilis can also affect the spinal cord, causing meningomyelitis. Meningovascular syphilis occurs 4 to 7 years after infection causing focal CNS ischemia or stroke. General paresis and tabes dorsalis occur later in the course of the disease, often decades after the primary infection. Paretic neurosyphilis causes a chronic progressive dementia. Tabes dorsalis symptoms include sensory ataxia, pain, optic atrophy, and autonomic dysfunction. Other presentations of neurosyphilis include uveitis, retinitis, and optic neuritis.
Diagnosis
Definitive diagnosis of syphilis is by direct detection of T. pallidum by examination of a smear or tissue from an active mucosal or cutaneous lesion using darkfield microscopy or DFA testing. Presumptive diagnosis of syphilis is by serology. Nontreponemal tests include the Venereal Disease Research Laboratory (VDRL) test and rapid plasma reagin (RPR) test. These tests are used primarily to screen asymptomatic patients and follow disease activity. Nontreponemal tests should not be used alone to diagnose the disease since false-negative and false-positive tests occur. False-positive nontreponemal tests occur with a variety of chronic conditions, usually at dilutions of less than 1:8. Antibody levels gradually decline in untreated patients, often reaching dilutions of less than 1:4 during late latent stages. In about one fourth of untreated patients the VDRL eventually becomes nonreactive. Specific treponemal tests include the fluorescent treponemal antibody absorption (FTA-ABS), the microhemagglutination T. pallidum (MHA-TP), and hemagglutination treponemal tests. These tests are used to confirm a positive screening test and once positive usually remain so for life. Neurosyphilis is diagnosed based on clinical and laboratory findings including cerebrospinal fluid (CSF) examination showing mononuclear pleocytosis, elevated CSF protein, and a positive CSF VDRL. A reactive CSF VDRL is sufficient to diagnose neurosyphilis, but a negative test does not exclude the diagnosis. The CSF VDRL is highly specific, with false positives occurring only with blood contamination of the CSF. Some experts recommend a FTA-ABS on the CSF to diagnose neurosyphilis. This test yields more false-positive tests, but some experts feel a negative test excludes the diagnosis of neurosyphilis. The serum VDRL is negative in up to 25% of patients with late neurosyphilis, but the treponemal tests remain positive.
Treatment
The recommended treatment for primary or secondary syphilis is with benzathine penicillin G (Bicillin LA, Permapen) 2.4 million units IM in one dose. For nonpregnant penicillin allergic patients treatment is with:
Doxycycline (Doryx, Monodox, Vibramycin, Vibra-Tabs) 100 mg po twice a day for 14 days or
Tetracycline (Sumycin, Tetracyn) 500 mg po four times a day for 14 days or
Erythromycin (E-Mycin, ERYC, Ery-Tab, PCE) 500 mg po four times a day for 14 days if compliance and follow-up are certain or
Ceftriaxone (Rocephin) 1 g once a day for 8 to 10 days with careful follow-up
Perform CSF and ocular slit-lamp examinations on patients with neurologic or ophthalmic disease and treat according to the results of these tests. Reexamine treated patients and perform quantitative nontreponemal testing 6 and 12 months after treatment. Patients with signs or symptoms of syphilis or who have a fourfold increase in the nontreponemal titer should be considered treatment failures or reinfected. Reevaluate these patients for HIV. Unless the patient is likely to be reinfected, perform a lumbar puncture to evaluate for neurosyphilis. Failure of the nontreponemal titer to decline fourfold within 6 months after treatment also identifies treatment failure. Reevaluate these patients for HIV and consider performing a CSF examination. At a minimum perform additional clinical and serologic follow-up on these patients and consider retreatment if follow-up cannot be assured. Retreatment is with three weekly intramuscular injections of 2.4 million units of benzathine penicillin G unless CSF findings suggest neurosyphilis.
Treatment of patients with early latent syphilis who have a normal CSF examination (if performed) is with benzathine penicillin G (Bicillin LA, Permapen) 2.4 million units IM once. For nonpregnant penicillin-allergic patients treatment is with:
Doxycycline (Doryx, Monodox, Vibramycin, Vibra-Tab) 100 mg po twice a day for 14 days or
Tetracycline (Sumycin, Tetracyn) 500 mg po four times a day for 14 days
Repeat quantitative nontreponemal testing at 6, 12, and 24 months after treatment. If titers increase fourfold, a titer of ≥1:32 fails to decline at least fourfold within 12 to 24 months, or signs or symptoms of syphilis develop, evaluate the patient for neurosyphilis and re-treat appropriately.
Treatment for patients with late latent syphilis or syphilis of unknown duration who have a normal CSF examination (if performed) is with benzathine penicillin G (Bicillin LA, Permapen) 2.4 million units IM weekly for 3 consecutive weeks. For nonpregnant penicillin-allergic patients treatment is with:
Doxycycline (Doryx, Monodox, Vibramycin, Vibra-Tab) 100 mg po twice a day for 28 days or
Tetracycline (Sumycin, Tetracyn) 500 mg po four times a day for 28 days
Repeat quantitative nontreponemal testing at 6, 12, and 24 months after treatment. If titers increase fourfold, a titer of ≥1:32 fails to decline at least fourfold within 12 to 24 months, or signs or symptoms of syphilis develop, evaluate the patient for neurosyphilis and re-treat appropriately.
Tertiary syphilis includes gummatous and cardiovascular syphilis, but not neurosyphilis. Perform a CSF examination on patients with symptomatic tertiary syphilis before treatment. Some experts recommend treating all patients with cardiovascular syphilis with a neurosyphilis regimen. The complete treatment of cardiovascular and gummatous syphilis is complex and should be done in consultation with experts. Treatment for tertiary syphilis is with benzathine penicillin G (Bicillin LA, Permapen) 2.4 million units IM weekly for 3 consecutive weeks. For nonpregnant penicillin-allergic patients treatment is with:
Doxycycline (Doryx, Monodox, Vibramycin, Vibra-Tab) 100 mg po twice a day for 28 days or
Tetracycline (Sumycin, Tetracyn) 500 mg po four times a day for 28 days
Little information exists on the proper follow-up of treated late syphilis. Clinical response depends on the nature of lesions present.
Neurosyphilis can occur at any stage of syphilis. Perform a CSF evaluation on patients with auditory symptoms, cranial nerve palsies, uveitis, neuroretinitis, optic neuritis, symptoms of meningitis, or other neurologic or ophthalmic symptoms. Treatment for neurosyphilis is with:
Aqueous crystalline penicillin G (Pfizerpen) 3 to 4 million units IV q4h for 10 to 14 days or
Procaine penicillin G (Wycillin) 2.4 million units IM per day plus probenecid 500 mg po four times a day, both for 10 to 14 days
An injection of benzathine penicillin G 2.4 million units IM after completion of neurosyphilis treatment is recommended by many experts. In patients with CSF pleocytosis, reexamine the CSF every 6 months until cell counts are normal. If the cell count does not decrease in 6 months or is not normal by 2 years, consider retreatment.
Prevention
Test all patients with syphilis for HIV. Presumptively treat individuals sexually exposed to a person with primary, secondary, or early latent syphilis within 90 days preceding the diagnosis even if seronegative. If the exposure was more than 90 days before the diagnosis, treat presumptively if serologic testing is not immediately available or if follow-up is uncertain. Patients with syphilis of unknown duration and nontreponemal serologic titers ≥1:32 may be considered as having early syphilis for purposes of partner notification and presumptive treatment of sex partners. Evaluate long-term sex partners of patients with late syphilis clinically and serologically and treat appropriately. Educate patients as previously described.
