Health Centers > HIV/AIDS Health Center > HIV and the Acquired Immunodeficiency Syndrom for professionals
HIV and the Acquired Immunodeficiency Syndrome for professionals
Introduction to HIV and Associated Disorders
The acquired immunodeficiency syndrome (AIDS), caused by the diabolically unique human immunodeficiency virus (HIV-1), has profoundly changed contemporary society and medical practice.
HIV and AIDS
- Introduction to HIV
- Immunology Related to AIDS
- The impact of HIV and AIDS
- Biology of Human Immunodeficiency Viruses
- Epidemiology of HIV infection
- Prevention of HIV infection
- Neurologic Complications of HIV-1 Infection
- Pulmonary Manifestations of HIV Infection
- Gastrointestinal Manifestations of AIDS
- Cutaneous Signs of AIDS
- Ophthalmologic Manifestations of AIDS
- Hematology/Oncology in AIDS
- Renal, Cardiac, Endocrine, and Rheumatologic Manifestations of HIV Infection
- Treatment of HIV infection and AIDS
- Management and Counseling for persons with HIV infection
The sections in this part enable the physician to understand the virus and its effects on humans. In addition, there is an extensive discussion of involvement of various organ systems, both by the virus itself and by opportunistic infections. The management of patients with HIV infection is presented in detail.
In 1981, the first cluster of cases of what we now call AIDS was recognized and reported. Nearly all of the early identified cases were in young homosexual men, but it was quickly learned that HIV infection could be transmitted by heterosexual contact and by blood transfer from infected to noninfected individuals.
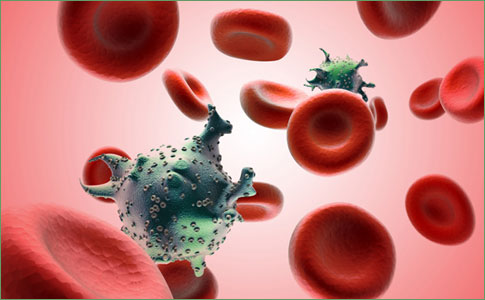
Immunology Related to AIDS
The clinical consequences of human immunodeficiency virus (HIV) infection are due to the ability of this retrovirus to disarm the host immune system, a process that occurs by virtue of the fact that the primary target for the virus is the helper-inducer subset of lymphocytes. This lymphocyte subset, defined by its surface expression of the CD4 molecule, acts as the pivotal orchestrator of a myriad of immune functions. HIV-1 infection can therefore be considered a disease of the immune system, characterized by the progressive loss of CD4-positive (CD4+) lymphocytes, with ultimately fatal consequences for the infected host.
Despite this immunosuppression induced by HIV, a number of specific immunologic defenses against the virus are generated in infected individuals and may contribute to the long, asymptomatic phase that follows infection by keeping the virus at least partially contained.
The potential significance of such responses is also underscored by the recent demonstration in animal AIDS models that a state of vaccine-induced protective immunity can be achieved against retroviruses related to HIV, and by the identification of infected persons who maintain control of HIV-1 viremia without drug therapy. An understanding of the immunology related to HIV provides insight not only into the clinical sequelae of infection, but also into the prospects for development of an effective vaccine against HIV.
AIDS HIV Prevention
If you know you are at high risk of HIV infection and come down with a bad case of the flu, see a doctor right away. It could be the early signs of HIV infection ...
The impact of HIV and AIDS
Over three decades have passed since the HIV and AIDS pandemic first came to world attention. Since then, it has had a devastating impact on the lives of individuals, families and communities and, as a consequence, on the social and economic development of countries where there are high numbers of people living with HIV and AIDS.
Progress is being made
But great progress has also been made during this time. People have come together to fight the epidemic. The 2012 UNAIDS World AIDS Day Report (PDF) shows that there were 700,000 fewer new HIV infections across the world in 2011 than in 2001.
The number of new HIV infections worldwide each year continues to drop and in a number of African countries the proportion of the population infected with HIV is declining. Particularly welcome is a steady reduction in the rate of transmission from HIV-infected pregnant women to their newborn children.
Quality of care and access to treatment available has improved enormously. There are now 8 million people receiving treatment for HIV.
Biology of Human Immunodeficiency Viruses
George M. ShawDiscovery of Human Immunodeficiency Viruses
The identification of HIV-1 as the causative agent of acquired immunodeficiency syndrome (AIDS) just 3 years after the clinical syndrome initially was described represents a remarkable scientific achievement that had its roots in earlier discoveries of animal and human retroviruses. The selective loss of CD4+ helper T lymphocytes in patients with the disease implicated an agent with T-lymphocyte cell tropism. As expected for an etiologic agent, HIV-1 was shown to be uniformly present in subjects with AIDS and to reproduce the hallmark of disease, destruction of T lymphocytes, in tissue culture.
Epidemiology of HIV infection and AIDS
Carlos del Rio, James W. CurranThe first cases of what has become known as the acquired immunodeficiency syndrome (AIDS) were reported in mid-1981 from Los Angeles, California. One month following these five reports of Pneumocystis carinii pneumonia (PCP) in young homosexual men, 26 cases of Kaposi's sarcoma (KS) in homosexual men in New York and California and additional cases of PCP and other opportunistic infections were reported. Reports of cases in the United States continued to rise, and soon the occurrence of PCP, KS, or other serious opportunistic infections in a person with unexplained immune dysfunction became known as AIDS. In retrospect, sporadic cases may have occurred in the United States, Europe, or Africa as much as three decades earlier, but the worldwide epidemic was not apparent until the 1980s.
The initial occurrence of AIDS in homosexual men and injecting drug users (IDUs) suggested by 1982 that a transmissible agent was the likely cause. The transmissible agent hypothesis gained credence by early 1983 with the documented occurrence of AIDS in persons with hemophilia and in recipients of blood transfusions. Within a year, the retrovirus, now termed human immunodeficiency virus (HIV), was isolated and shown to be the cause of AIDS.
Recent data support the theory that the HIV virus originated in Africa. Blood obtained in 1959 from an adult Bantu man in the Democratic Republic of Congo represents the oldest known HIV-1 virus infection.
- AIDS and HIV infection outside the United States
- Epidemiology of HIV infection and AIDS
- HIV infection and AIDS in the United States
- Indicence and trends of AIDS in the United States
- Modes of HIV Transmission
- Other Modes of Transmission
- Perinatal Transmission
- Prevalence and Incidence of HIV Infection in the United States
- Transmission in the Health Care Environment
- Transmission Through Parenteral Exposure to Blood or Blood Products
Prevention of HIV infection
Michael S. SaagPrevention of HIV infection requires a thorough understanding of the modes of viral transmission, the populations at risk, and the established guidelines to avoid high-risk exposures. HIV has been identified in virtually every body fluid and tissue, including blood, semen, vaginal secretions, saliva, tears, breast milk, cerebrospinal fluid, amniotic fluid, urine, and fluid obtained from bronchoalveolar lavage. In most instances, the virus resides in lymphocytes present within body fluids; therefore, any fluid that contains lymphocytes could be implicated theoretically in the spread of the virus. Nonetheless, no cases of HIV transmission have been documented through any body fluids except blood and fluids grossly contaminated with blood, semen, vaginal secretions, and, rarely, breast milk. HIV has been transmitted through transplanted organs, including kidney, liver, heart, pancreas, and bone.
Neurologic Complications of HIV-1 Infection
Richard W. PriceThe neurologic complications of HIV-1 infection are both common and varied. Indeed, only rarely do the central and peripheral nervous systems of HIV-infected patients remain unaffected through the course of untreated disease. Because each of the individual neurologic disorders is discussed in more detail elsewhere in this volume, the major purpose of this section is to provide an overview and a general guide to diagnosis and management.
Although the major susceptibility to neurologic complications occurs in the late phase of HIV-1 infection, at the time when immunosuppression leads to a marked increase in vulnerability to a host of conditions, patients may also manifest certain neurologic afflictions early in infection. Because the neurologic complications of early and late HIV-1 infection differ, they are considered separately. Indeed, because of these stage-related differences in susceptibility, when approaching diagnosis in HIV-infected patients it is important to characterize their "background" systemic HIV-1 infection, either clinically with respect to the presence or absence of previous opportunistic infections indicating compromised immunity or by assessment of surrogate markers, particularly the blood CD4+ lymphocyte count. Emerging data suggest that susceptibility to late neurologic complications can be delayed or reversed by highly active antiretroviral therapy (HAART), sustaining the value of the CD4+ count in predicting disease vulnerability.
- Early HIV-1 Infection
- Effects of HIV-1 on the Nervous System
- Late HIV-1 Infection
- Meningitis and Headache
- Myelopathies
- Myopathies
- Neurologic Complications of HIV-1 Infection
- Opportunistic Neoplasms
- Opportunistic Nervous System Infections
- Peripheral Neuropathies
- Predominantly Focal Brain Disorders
- Predominantly Nonfocal Brain Disorders
Pulmonary Manifestations of HIV Infection
Philip C. HopewellLung disease, specifically Pneumocystis carinii pneumonia (PCP), was the first recognized mode of expression of infection with the human immunodeficiency virus (HIV). Since the original clusters of cases of PCP were reported in 1981, the respiratory system has continued to be a common site of involvement in persons infected with HIV. Although pulmonary disorders are more frequent among persons who have advanced immunosuppression, meeting the current surveillance definitions for the acquired immunodeficiency syndrome (AIDS), lung diseases also occur with an increased frequency in individuals with HIV infection who have lesser degrees of immunosuppression. This section describes the relative frequency and spectrum of lung diseases that occur among persons infected with HIV and focuses on the approach to evaluating symptoms that originate from the respiratory tract in this unique group of patients.
- An Integrated Approach to Diagnosis
- Clinical features of HIV-Associated Disorders of the Respiratory Tract
- Correlation of Respiratory Tract Disorders with stage of HIV disease
- Disorders Associated with Severe Immune Suppression
- Effects of HIV on Respiratory Tract Defenses
- Preventing Lung Diseases in Persons with HIV Infection
- Pulmonary Manifestations of HIV infection
- Relationship of respiratory tract diseases to CD4+ Lymphocyte count, Demographic Characteristics, and Transmission Category
Gastrointestinal Manifestations of AIDS
John G. BartlettThe gastrointestinal tract is an especially common site for clinical expression of human immunodeficiency virus (HIV) infection and is an important factor in morbidity from opportunistic infections in late-stage disease, as well as gastrointestinal complications from antiretroviral agents or other drugs. Nearly all opportunistic infections occur when the CD4 count is less than 200/mm3 , and almost all seem to respond well to immune reconstitution when achieved with antiretroviral therapy.
Cutaneous Signs of AIDS
Neal S. PenneysCutaneous signs and symptoms associated with acquired immunodeficiency syndrome (AIDS) increase in frequency and severity as the disease advances. However, infection by human immunodeficiency virus (HIV) may produce a transient macular roseola-like eruption. As HIV infection progresses, infectious processes and neoplastic disease are most often seen. Patients also may have symptoms such as pruritus without visible skin lesions.
Cutaneous infections are a common feature of AIDS. Superficial infections such as dermatophytosis, candidiasis, and scabies may be extensive and have altered appearances. Superficial fungal infections may coexist with other pathogens such as herpesvirus or cytomegalovirus to produce unusual complex cutaneous infections.
Ophthalmologic Manifestations of AIDS
Mark A. Jacobson M.D.Infectious or noninfectious ocular disorders, some of which may lead to severe visual impairment, have been reported in 40 to 90% of patients with acquired immunodeficiency syndrome (AIDS) referred for formal ophthalmoscopy. In prospective observational cohort studies conducted prior to the clinical availability of the new, more potent generation of antiretroviral agents for the treatment of human immunodeficiency virus (HIV) disease, the incidence of cytomegalovirus (CMV) retinitis (the most common ophthalmologic complication of AIDS) was reported to be in the range of 20 to 40% in patients with an AIDS diagnosis. In the first 18 months since potent HIV protease inhibitors became widely available in the United States and Europe, the incidence of new CMV retinitis diagnoses decreased markedly. How sustained this decrease will be is unknown, but if new antiretroviral treatment strategies ultimately lead to extensive HIV cross resistance to these agents, the incidence of CMV retinitis may again increase.
The differential diagnosis of HIV-associated ocular disease is best considered by its anatomic location.
Hematology/Oncology in AIDS
David T. ScaddenJerome E. Groopman
A signature abnormality of human immunodeficiency virus (HIV) infection is the decline in the number of CD4 lymphocytes over time. However, other cytopenias also are seen in advanced disease, with anemia reported in 60%, thrombocytopenia in 40%, and neutropenia in 50% of patients with acquired immunodeficiency syndrome (AIDS). These cytopenias occur in conjunction with progressive deterioration of immune function and are less common in the earlier stages of HIV infection or in patients responding to antiretroviral medications. Thrombocytopenia is the exception and may constitute a manifestation of HIV infection during the asymptomatic phases. Multiple contributing factors frequently are operative in the cytopenia in advanced HIV infection, including direct and indirect effects of HIV; opportunistic infections; neoplasms; and toxic antiretroviral, antimicrobial, or antitumor chemotherapy. Evaluation of patients with low blood counts should focus on infectious processes and attendant myelotoxic effects of therapy. In addition to the usual laboratory approaches to cytopenia based on impaired production, excess consumption, and/or sequestration, a number of other diagnostic studies should be considered. These include blood isolator cultures for fungi and mycobacteria, and serum assessment for cytomegalovirus (CMV) antigen or IgM antibody to parvovirus.
Although the utility of bone marrow aspirate and biopsy in an HIV-infected patient with low blood counts has been debated, morphologic changes such as giant pronormoblasts in parvovirus infection and special stains for mycobacteria and fungi may hasten identification of a reversible cause of myelosuppression. Marrow sampling is not more sensitive, however, than routine microbiologic tests in diagnosing these abnormalities.
Morphologic abnormalities of myeloid and erythroid lineages often are present in the bone marrow of patients with HIV disease in the absence of infection or neoplasm. These changes are nonspecific and include hypercellularity, dysplasia with frequent megaloblastosis, lymphoid aggregates, and increased plasma cells and reticulin. The pathogenetic mechanisms for these morphologic abnormalities and the associated impaired hematopoiesis are not well defined. Laboratory studies of hematopoiesis in HIV infection have yielded variable and differing results. The bulk of evidence suggests that HIV does not directly infect early progenitors but may alter the proliferative capacity of progenitors by two possible mechanisms: (1) induction of inhibitory factors in the marrow microenvironment, or (2) interaction with the progenitor cell surface and induction of cell death (apoptosis) without infecting stem cells.
Renal, Cardiac, Endocrine, and Rheumatologic Manifestations of HIV Infection
Michael S. SaagInfection with the human immunodeficiency virus type I (HIV) is a multisystem disease. Manifestations of pulmonary, gastrointestinal, neurologic, hematologic, and oncologic disease are well described in the literature, owing mainly to their high prevalence and often dramatic modes of presentation. In contrast, HIV-related renal, cardiac, endocrine, and rheumatologic diseases are more insidious in presentation. As overall survival of HIV-infected individuals continues to improve and therapeutic regimens become more sophisticated, clinicians will undoubtedly encounter disorders of the latter organ systems with increasing frequency.
Treatment of HIV infection and AIDS
Robert YarchoanSamuel Broder
Since the identification of the acquired immunodeficiency syndrome (AIDS) as a new entity in 1981, dramatic changes have occurred in therapy for this disease and its related disorders. In 1984, therapy was either entirely supportive or directed at a bewildering array of infectious and oncologic complications. The identification of human immunodeficiency virus (HIV) as the causative agent of AIDS and the elucidation of its life cycle have enabled the development of specific antiretroviral therapy, and such therapy is now recognized as being the cornerstone of treatment for HIV infection and AIDS. Substantial advances have been made over the past several years. At least 13 antiretroviral drugs are now approved belonging to three major classes: nucleoside reverse transcriptase inhibitors (NRTIs), non-nucleoside reverse transcriptase inhibitors (NNRTIs), and protease inhibitors (PIs).
It has also been shown that these drugs are particularly effective if used in combination regimens that effectively suppress HIV replication. The physician treating HIV-infected patients thus has a wide array of active regimens to chose from; and although none is curative, the use of these drug regimens has substantially improved the outlook for HIV-infected patients. At the same time, however, these recent developments have increased the complexity of therapy, and it has been shown that the experience of physicians in treating AIDS has a direct bearing on their patients' survival. It is thus essential that physicians setting out to treat HIV-infected individuals have a good understanding of the issues involved. In this section, the principles underlying the therapy for HIV infection, the drugs used, the approaches now being used, and the limitations of these approaches are discussed. It should be noted, however, that this is an extremely rapidly moving field and that physicians treating HIV-infected patients should make a particular effort to stay informed of new developments.
- Drugs used in the treatment of HIV infection
- General Recommendations for the treatment of HIV infection
- Immune Reconstitution and other Approaches
- Non-Nucleoside Reverse Transcriptase Inhibitors
- Principles and Goals for the treatment of HIV infection
- Protease Inhibitors
- Treatment of HIV Infection and AIDS
- Treatment of the Pregnant HIV-Infected Patient
Management and Counseling for persons with HIV infection
John A. BartlettTreatment advances in human immunodeficiency virus (HIV) disease have dramatically changed the management of chronically infected persons. Advances in three areas have contributed to these successes: (1) an improved understanding of the dynamic nature of HIV replication and its implications for treatment, (2) the technology to measure HIV RNA levels with an understanding of their correlation with prognosis in untreated and treated persons, and (3) the availability of an expanding number of antiretroviral agents with increased potency. These advances have resulted in profound virologic suppression in treated patients with an associated improvement in clinical outcomes and survival. However, despite these treatment advances, significant gaps remain in our understanding of the strategies needed to guide treatment initiation, and when to change a failing regimen. Coincident with these treatment advances, persons with HIV infection in the United States are increasingly impoverished, more likely to abuse drugs, and have less access to health care. The use of complex antiretroviral regimens has created a scheduling challenge for many patients, and the success of therapy is absolutely dependent on patient adherence. Therefore, health care providers must carefully assess the resources and commitment of persons beginning antiretroviral therapy, design a highly potent and convenient regimen for individual patients, optimize adherence through patient preparation and education, and continually reassess the entire process in a patient on treatment. Significant questions remain unanswered regarding the durability of successful antiretroviral therapy, the potential infectivity of persons on treatment, and the optimal management of treatment failure. These uncertainties may make counseling difficult because individual patients may experience emotional extremes in periods of treatment successes and failures.
